
Behavioral health treatment plans are an important tool, both for providers and patients. A treatment plan is a roadmap that describes where your patient is right now, where they are going, and how they’ll get there. This makes the treatment plan an effective behavioral health practice cornerstone.
In plain language, a behavioral health treatment plan connects the patient’s diagnosis and current needs to specific goals, measurable objectives, clinical interventions, timelines, and methods for tracking progress. It should be collaborative, individualized, and updated as the patient’s needs change.
What is a Treatment Plan?
A behavioral health treatment plan includes basic patient information, patient behavioral health concerns, treatment goals, step-by-step objectives for reaching each goal, selected interventions, and measurement criteria for progress and outcomes. A treatment plan is a versatile document that reflects the patient and their needs. It provides structure and direction for the patient’s care, and it should be updated periodically.
A diagnosis and a treatment plan aren’t the same thing. A diagnosis identifies the condition or symptoms being treated, while the treatment plan explains what the patient and clinician will work toward and how they’ll measure progress. The diagnosis helps inform the plan, but it doesn’t replace it.
Components of a Behavioral Health Treatment Plan
Although treatment plans vary widely, they usually have the following four sections:
1. Assessment and Diagnosis
This section explains how assessment data informs the treatment plan. This includes intake data, psychosocial history, description and history of symptoms, and past and present diagnoses.
Arriving at an accurate diagnosis is extremely important. Past diagnoses may have been wrong or incomplete. Providers want to explain the assessments performed and resulting diagnosis in this section of the treatment plan.
The diagnosis establishes the clinical context, but the rest of the treatment plan translates that information into an individualized course of care. Two patients with the same diagnosis may need different goals, interventions, timelines, and measures of progress.
2. Treatment Goals and Objectives
Patients often come with knowledge of what is wrong, but they may not know where they want to be in terms of behavioral health goals, and they are even less likely to know how to get there. Strong treatment plans include patient involvement in setting measurable treatment goals, including “chunking” into smaller objectives that are more actionable and manageable.
The provider should steer the patient toward treatment goals and objectives that are SMART:
- Specific
- Measurable
- Attainable
- Relevant
- Time-bound
Some objectives may be broken down into smaller steps, such as specific actions a patient can take when facing anxiety. The patient may want to refer to this section in their daily life, and it’s often necessary to reference it in sessions.
Goals describe the broader outcomes the patient wants to achieve. Objectives identify the specific, measurable steps that move the patient toward those outcomes. For more examples, review this guide to mental health treatment plan goals and objectives.
Some clinicians like to call this section a treatment “contract.” This can help strengthen the commitment of the patient to follow through on the plan. Treatment goals and objectives, as well as treatment contracts, can be vital to successful goal achievement.
3. Interventions and Strategies
Select several interventions and strategies (preferably evidence-based) to help the patient achieve their goals. Interventions can include types of therapy that will be used in client sessions, such as cognitive behavioral therapy, narrative therapy, strengths-based therapy, or other methods. Interventions can also include psychoeducation, materials and resources, progress monitoring, and medications.
Strategies, such as deep breathing exercises when encountering stress, will need to be taught to the patient. This may include demonstration by the clinician, so the patient remembers to use the strategy in their daily life when they need it. Interventions and strategies are not one-size-fits-all; it’s best to modify them to fit each patient’s needs.
Choose interventions by considering the patient’s diagnosis, symptoms, goals, strengths, preferences, culture, access needs, and response to care. You’ll also want to consider the treatment setting. For virtual care, select interventions that can be delivered effectively through telehealth and practiced safely between sessions.
The treatment plan should explain how each intervention connects to a goal or objective. This keeps the plan clinically meaningful instead of turning it into a list of disconnected techniques.
4. Timeline and Progress Monitoring
Timeframes are a key part of treatment plans. Make progress monitoring a part of each appointment.
It can include patient data submitted electronically through a patient portal, or patients can provide the necessary information at each appointment. This helps reduce the number of appointments. Of course, the provider will want to make sure it aligns with expectations for the patient.
Treatment goals should all have timeframes, but these timeframes are not set in stone. Progress monitoring determines if adjustments need to be made.
Review the treatment plan regularly during care and update it whenever the patient’s goals, diagnosis, symptoms, level of care, or response to treatment changes. Formal review requirements may also vary by payer, program, state, and practice policy, so your workflow should make deadlines and review cycles easy to track.
For telehealth patients, practices can collect assessments or outcome measures before the virtual visit, review progress during the session, and update the plan without shifting to a separate paper-based process.
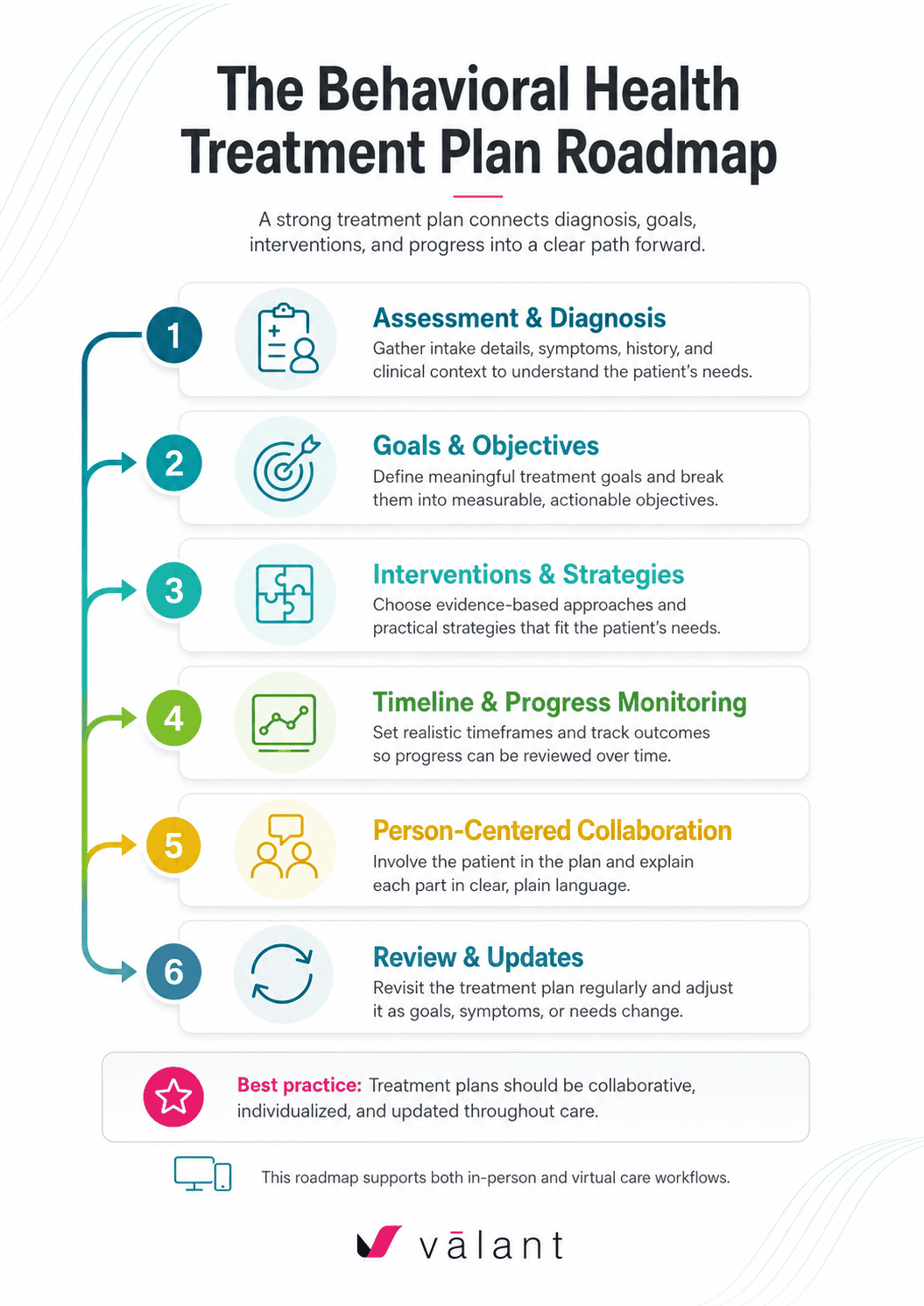
Person-Centered Planning
Your patient should be closely involved in planning their treatment. You are only with them for appointments occasionally, but the patient lives with and uses the treatment plan daily. Person-centered planning does not mean that you let the patient write their own treatment plan, but rather that you involve them in each step, carefully explaining why you are recommending certain goals, interventions, strategies, and timelines.
Make the treatment plan collaborative and offer patient choice when appropriate. This will help the patient gain understanding and stay engaged. At the same time, you are the expert; draw on your training and experience.
When explaining a treatment plan, use plain language instead of clinical shorthand. You might describe it as a shared roadmap that outlines what the patient wants to change, the smaller steps you’ll work on together, and how you’ll know whether treatment is helping.
During a telehealth visit, you can review the plan together on screen, talk through each section, and pause for questions. The technology shouldn’t make the conversation feel scripted. It should give you a clear structure for keeping the patient involved.
Cultural Competence and Diversity
Don’t underestimate the importance of cultural sensitivity in treatment planning. Many cultures still have a stigma attached to behavioral health, so it’s important to address this and be discreet when needed.
Tailor treatment plans for diverse populations. Good strategies include learning about the cultures and religious views of the patients you serve. You may even want to organize staff training programs.
In addition, it’s generally better to ask questions of patients, rather than making assumptions. Work with your patients to adapt their treatment plans to their cultural and religious needs.
Also consider whether language, technology access, disability, health literacy, or comfort with telehealth may affect how the patient participates in treatment. These factors may shape the interventions you select and how you communicate the plan.
Legal and Ethical Considerations
It’s important to regularly obtain informed consent from patients and to keep their treatment plan confidential except when disclosure is appropriate. As a provider, you have legal and ethical obligations, such as safeguarding patients’ protected health information, compliance with HIPAA, and a duty to report specific threats to others or themselves.
You also have an ethical obligation to offer the patient effective treatment tailored to their needs that benefits their behavioral health. A well-written behavioral health treatment plan is a great way to help with this.
When treatment planning takes place through telehealth, confirm that the patient is in an appropriate private setting and use secure technology for discussing, storing, and sharing treatment information. The same documentation, confidentiality, and informed-consent responsibilities still apply in virtual care.
Challenges in Treatment Planning
Several common challenges faced by behavioral health professionals and clinicians include writing the treatment plan, tailoring it to the patient, and following through on it. These are not surprising, and patients themselves face many of the same issues. The treatment plan is not something likely to be completed on the first visit, but you’ll want it in place relatively quickly, so that you can make progress.
Clinicians often struggle with treatment-planning documentation because they are balancing clinical judgment, payer requirements, individualized language, measurable objectives, and limited time. Starting from scratch, entering the same information in multiple places, and keeping review deadlines organized can add even more administrative pressure.
The right software can help improve the process. Oftentimes, working with an EHR-integrated behavioral health treatment plan is easier and more efficient than paper.
Look for a solution that will pre-fill information received via intake forms and other sources. Starting with a treatment plan template, rather than writing one each time from scratch, is another time saver.
Flexible templates and evidence-based content can give clinicians a strong starting point while still allowing them to personalize the plan. For growing organizations, standardized workflows can also improve consistency across providers without forcing every clinician to use identical language. Learn more about saving time and effort when managing counseling treatment plans at scale.
It’s important to be intentional about revisiting the treatment plan at each appointment, even if only to remind the patient of their goals and of how far they’ve progressed already.
Documenting and Updating Treatment Plans
Accurate documentation is essential. Update your patients’ treatment plans periodically, based on notes and assessments. Keep a close eye on the indicated timeframes for treatment goals and emerging patient needs. Establishing consistent routines and keeping up with documentation can be critical to outcomes.
A strong workflow should help you see which plans are due for review, connect progress notes to treatment goals, and document why goals, objectives, or interventions have changed. That creates a clearer clinical record and makes the plan more useful during ongoing care.
Rather than treating updates as a separate administrative exercise, build them into your regular sessions. Even a brief review can help you confirm whether the plan still reflects the patient’s priorities and progress.
Integrating Technology
Modern treatment planning includes telehealth technology for virtual therapy sessions, clinical documentation, and medication management. Some of these technologies are client-facing, some are only for practice staff, and some are both.
An integrated behavioral health EHR can keep intake information, diagnoses, progress notes, assessments, treatment plans, and review dates connected in one workflow. That can reduce duplicate entry and make it easier to build or update a plan during both in-person and telehealth visits.
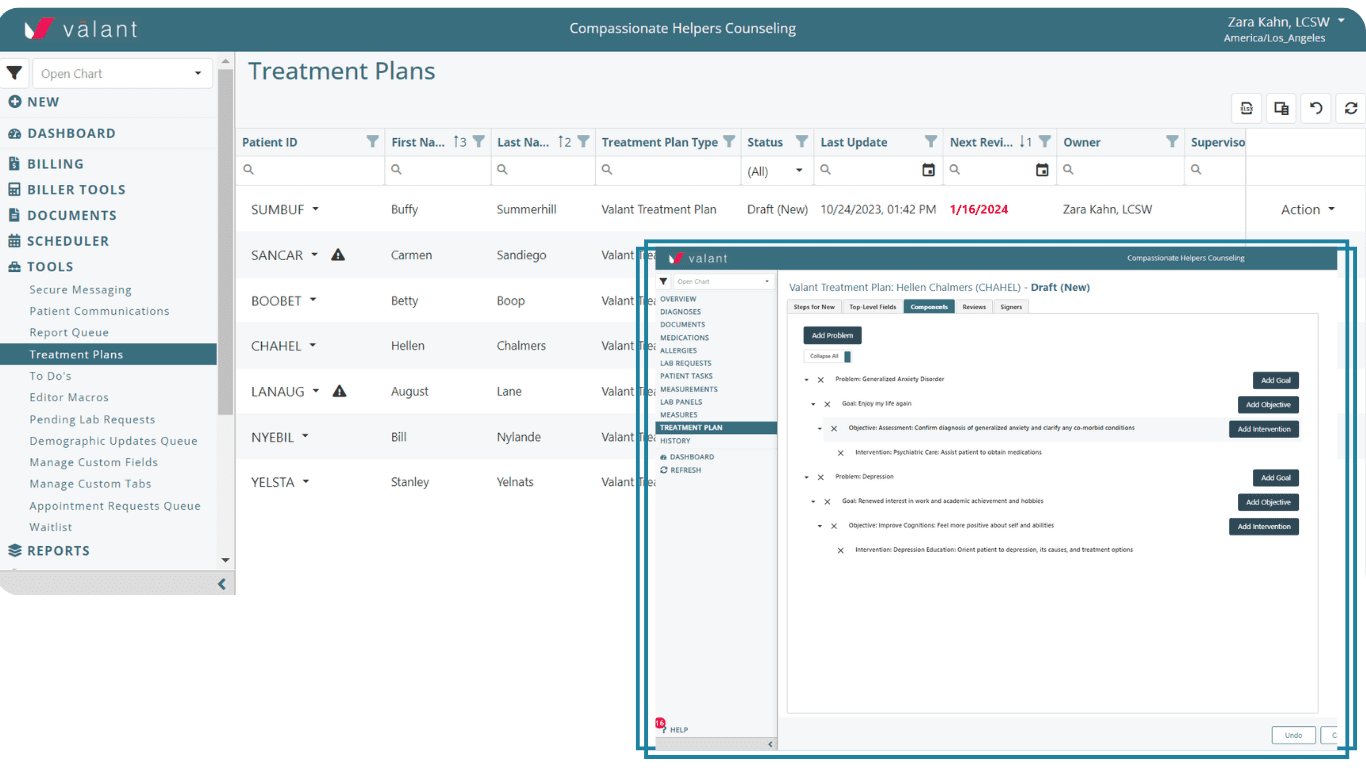
When evaluating behavioral health treatment-planning software, look for configurable templates, measurable goals and objectives, customizable intervention libraries, review-cycle reminders, progress tracking, and workflows that support collaboration among clinicians, supervisors, and patients.
Not every patient is comfortable with technology, but even for such patients, providers and staff can use technology to create effective treatment plans. Although there’s no substitute for patient interaction, don’t forget: tools that help you save time on other tasks will free up more time to spend with your patients.
Turn Treatment Plans Into a Clear Path Forward
Consider how to make comprehensive, person-centered treatment planning your goal. This can lead to improvement in quality of care, and your patients will see the positive outcomes in their day-to-day lives.
The strongest treatment plans connect diagnosis, goals, objectives, interventions, timelines, and progress measures in language the patient can understand. When your documentation workflow supports that process instead of slowing it down, you can spend more time making the plan meaningful and less time managing paperwork.
Explore Valant’s mental health treatment-planning tools to see how flexible templates, evidence-based content, and connected clinical workflows can support more efficient, collaborative care.







